
I believe that expenditure on prevention should not lie with the "health system". That system will always be focused on cure and rightly so. So many of the preventative factors are more social than clinical, therefore they should be managed through systems and structures that are focused on place-based, community-based and community-led activities.
- AHP Panellist
Too many people do not have the emotional energy to engage in preventive health measures because they are time poor. Giving people more time in their lives through telehealth, working from home, more locally-based services/employment/shops would help give people the space to focus on preventive health measures such as cooking nutritious meals and exercising.
- AHP Panellist
For December 2020 and January 2021 Australia’s Health Panel (AHP) looked at the Australian Government’s draft “National Health Prevention Strategy”. As a member of the Expert Steering Group for the Strategy, CHF sought to gauge the consumer view about the draft Strategy, and preventative health more broadly. This will help shape our advocacy as part of the Steering Group as the Strategy is finalised and begins implementation.
Demographics
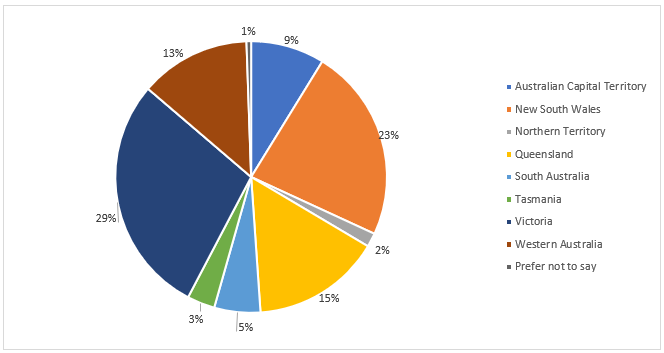
This Australia’s Health Panel survey had 188 panellists participate. They were mostly female (78%) and skewed older with 39% aged 46-65 and 41% aged over 65. Nearly two thirds (63%) of the participating panellists lived in major cities (more than 250,000 people) and they hailed from all states and territories of Australia (see Figure 1).
Fig 1: NatPrevHealth survey - graph
Participating panellists self-reported being in good health, with 68% being in either excellent or good health. Over one in five (22%) identified as a person with a disability (PwD) and nearly one in ten (9%) identified as LGBTIQA+. Five percent identified as culturally and linguistically diverse (CALD) and 2% as Aboriginal or Torres Strait Islander.
Factors impacting health in Australia
The majority (59%) of panellists either disagreed or strongly disagreed with the idea that individuals were solely responsible for maintaining their own health and preventing disease, with an overwhelming majority (96%) agreeing that the ability for consumers to live healthy lives was significantly impacted by the conditions they live and work in (see Table 1). A similar majority (89%) agreed that they personally were impacted by the conditions they live and work in. Majorities of panellists also agreed or strongly agreed that factors outside the health system such as income, education and the environment significantly impact both the ability of the general consumer to live a healthy life (90%) and their personal ability to live a healthy life (88%). A similarly overwhelming majority (94%) agreed that Government has a responsibility to promote conditions that support individuals leading healthy lives. Collectively these show strong acceptance amongst of Australian community of the existence of external factors which impact on an individual’s health, understanding that they are beyond their individual control and the belief that the government has a responsibility to address those external factors.
|
Strongly agree |
Agree |
Neither agree nor disagree |
Disagree |
Strongly disagree |
Don't know |
Question |
|---|---|---|---|---|---|---|
|
7% |
19% |
14% |
34% |
25% |
1% |
Everyone is solely responsible for maintaining their own health and preventing disease. |
|
43% |
46% |
2% |
6% |
3% |
1% |
My ability to live a healthy life is significantly impacted by the conditions that I live and work in. |
|
55% |
41% |
3% |
1% |
0% |
0% |
Consumers’ abilities to live healthy lives are significantly impacted by the conditions they live and work in. |
|
48% |
30% |
8% |
9% |
4% |
0% |
Factors outside of the health system (such as income, education and the environment) significantly impact my ability to live a healthy life. |
|
63% |
27% |
4% |
2% |
2% |
1% |
Factors outside of the health system (such as income, education and the environment) significantly impact on people's ability to live healthy lives. |
|
66% |
28% |
2% |
2% |
1% |
1% |
Governments have a responsibility to promote conditions that support individuals in leading healthy lives. |
|
48% |
47% |
4% |
0% |
0% |
0% |
I have a good understanding of what behaviours can improve my health and prevent disease. |
|
1% |
23% |
24% |
43% |
5% |
2% |
Most consumers have a good understanding of what behaviours can improve their health and prevent disease. |
|
30% |
49% |
11% |
7% |
2% |
0% |
I am able to adopt behaviours that can improve my health and prevent disease. |
|
1% |
29% |
25% |
35% |
7% |
2% |
Most consumers are able to adopt behaviours that can improve their health and prevent disease. |
|
28% |
41% |
10% |
16% |
4% |
1% |
It is easy for me to find reliable and trustworthy information to support my health and well-being. |
|
1% |
15% |
25% |
41% |
15% |
2% |
It is easy for most consumers to find reliable and trustworthy information to support their health and well-being. |
|
2% |
10% |
14% |
32% |
36% |
6% |
Australia's health system currently has the right balance between preventing illness & disease and treating illness and & disease. |
Panellists had divergent views as to the ability of consumers in general to affect their own health compared to the panellist’s personal ability to affect their own health (as shown in Table 1). A minority of panellists agreed that most consumers have a good understanding of what behaviours can improve their health and prevent disease (24%), that most consumers could adopt behaviours that improve their health & prevent disease (30%) or easily find reliable & trustworthy information to support their health and well-being (16%). This finding aligns with prior research looking into the health literacy levels of Australians which has found that health literacy levels are low and reinforces the need for specific support to be provided to allow people to effectively engage with their health and improve their health status.
Conversely, most panellists agreed that they personally had a good understanding of what behaviours can improve their health and prevent disease (95%), could adopt behaviours that improved their health and prevent disease (79%) and easily find reliable and trustworthy information to support their health and well-being (69%). This large discrepancy could be due to several different factors. In particular, it could be an artefact of selection bias, where those members of the Australian public who have signed up to participate in Australia’s Health Panel are a self-selecting group who have higher health literacy and health knowledge, leading to them outperforming the average Australian on these measures. Equally, it could be a manifestation of the cognitive bias known as ‘Illusory Superiority’ where a person overestimates their own abilities and skills compared to what they believe others are able to do. While it is not possible to identify the precise cause of the discrepancy between the views of panellists here from the data gathered, it does serve as a prescient reminder for advocates and policy-makers that such cognitive biases need to be considered and taken into account. People may believe that they are doing the ‘right’ thing in terms of gathering reliable information and establishing healthy behaviours but inadvertently be doing things that are less than optimal.
Of note is that only 12% of panellists believed that the current Australian health system has gotten the balance right between ‘preventing illness and disease’ and ‘treating illness and disease’, showing strong community support for reviewing and changing how we currently approach preventative health.
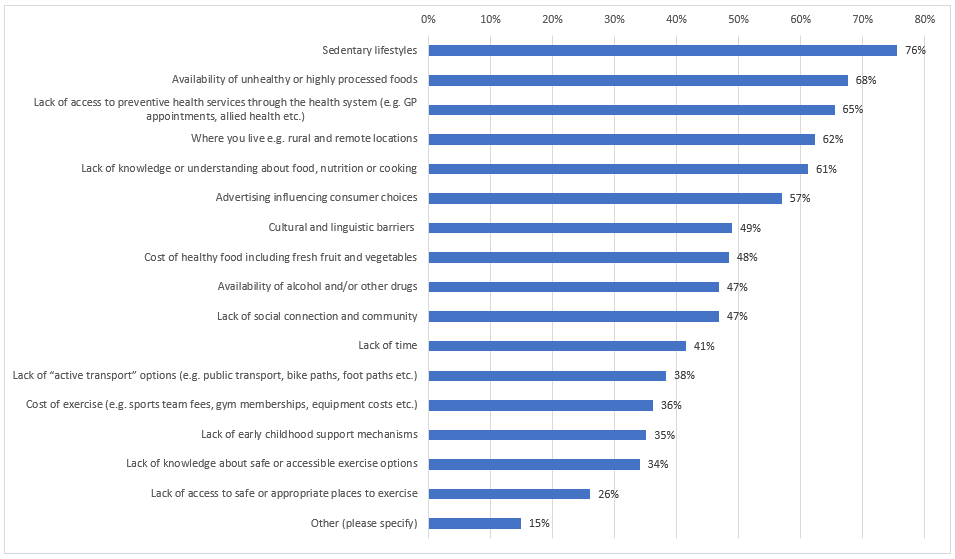
When asked what the key barriers were towards maintaining a healthy life, six of the pre-defined items were identified as a key barrier by the majority of panellists (see Figure 2). They were sedentary lifestyles (75%), the availability of unhealthy and highly processed foods (68%), lack of access to preventative health services (65%), where you live e.g. rural and remote locations (62%), a lack of knowledge or understanding about food, nutrition and cooking (61%) and advertising (57%).
This suggests that these six barriers should be priority areas the National Health Preventative Health Strategy looks to address, as they affect large numbers of consumers. However, it should be noted that of the other 10 barriers provided, nine of them were identified as key barriers by at least one third to almost one half of panellists. This suggests that all the barriers play a role in impeding the health status of many Australians and will also need to be effectively addressed as part of the National Health Prevention Strategy. Ultimately this indicates that there is no silver bullet single barrier that can be overcome to fix the problems in the current system and that a multi-faceted approach that is wide-ranging will be needed.
Fig 2: graph - NatPrevHealth survey
When given the option to nominate additional barriers panellists perceived to exist, a repeated view was that fundamental parts of the Australian health system were not designed to facilitate preventative care. The systemic barriers included: a lack of bulk-billing access to preventative interventions; a lack of clarity around what preventative services were available; attitude of health practitioners not supporting; insufficient time in GP appointments to address all of someone’s issues, and a general focus on curing rather than prevention. In addition to these system-wide barriers, the attitudes of people as individuals were another barrier that needed to be overcome. This includes: people thinking that they are ‘invincible’ and do not personally need to take precautionary measures; people thinking that minor ailments can be ignored with no risk, and a general taboo against mental health. The last commonly identified one was one of affordability and poverty with the costs of accessing preventative healthcare being prohibitive for those who are unable to take time off work or pay out of their own pocket for non-bulk-billed services. This often leads to major problems down the road that costs more for both the consumer and the health system.
Our preventive health system in Australia is geared to middle-class affluent families. There needs to be an approach that supports prevention across the lifespan and in all socio-economic and cultural groups. This includes, for example, prioritising parks and sports grounds for exercise in ALL suburbs, rather than gobbling them up with development or not maintaining them and letting them become unsafe and unattractive.
- AHP Panellist
Attitudes towards the draft National Preventative Health Strategy
When asked about the target of 5% of the National Health Budget being allocated to preventative health measures, only 31% of panellists thought that that target seemed about right. The majority (57%) thought that 5% was too low while a further 9% were unsure. Only 3% thought that the target seemed too high. Similarly only 34% thought that the target of 10% of the Medical Research Future Fund grants funding preventative health research seemed about right, with 46% thinking it was too low, 10% being unsure and 9% thinking it is too high. This indicates strong support in the community for increased funding for preventative health and preventative health research, beyond what the National Health Prevention Strategy is currently proposing.
An overwhelming majority of panellists believed it was important for the government to allocate funding of preventative health measures based on independent expert advice, with 75% strongly agreeing and a further 19% agreeing. This shows the importance of clearly embedding expertise into transparent and independent decision-making processes when allocating funds in the healthcare space. Not only to ensure that funding is allocated optimally but to give the Australian public the confidence that funding is being allocated optimally.
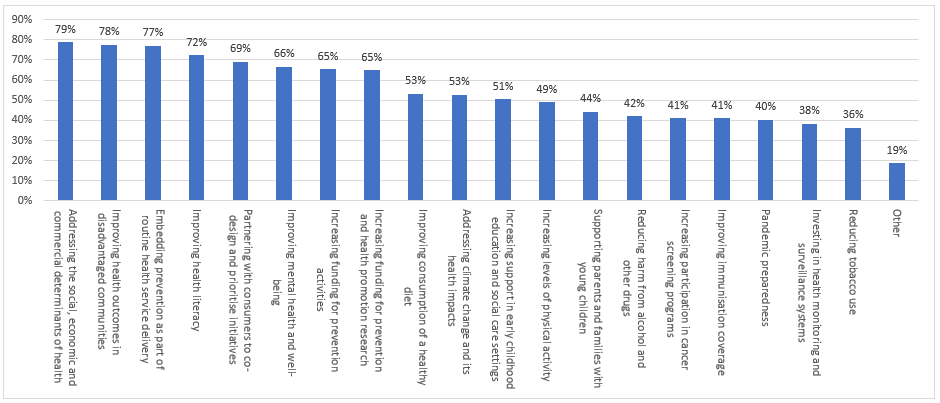
When asked what the priorities of the National Preventative Health Strategy should be, four priorities received over 70% support among panellists (see Figure 3). They included: ‘addressing the social, economic and commercial determinants of health’ (79%); ‘improving health outcomes in disadvantaged communities’ (78%); ‘embedding prevention as part of routine service delivery’ (77%), and ‘improving health literacy’ (72%).
Each of these in turn represents a desire to fundamentally reshape how healthcare is delivered in Australia: recognising that factors beyond a person’s control can affect their health; ensuring that those who are currently being left behind are given the extra support needed; making preventative care the expected standard of ordinary care where it is not novel, and giving people the skills and abilities to fully engage with their own healthcare options.
Fig 3: graph - NatPrevHealth survey
Panellists were then given a list of commonly proposed preventative health measures and asked which they would support being included as part of the implementation of the Strategy, with seven of the 13 listed measures being supported by the majority of panellists (see Figure 4). The most popular one, with 79% support, was placing restrictions on advertising and promotional campaigns for highly processed and unhealthy foods, especially those targeting children. When considering that 60% of panellists also supported mandatory inclusion of ‘health star rating’ of packaged food, there is evidently community support for changing the information that is being provided to consumers by food companies. Allowing consumers to have better capacity to make informed decisions when considering their food choices. There is also community support for government intervention in the pricing of foods as part of preventative health, with majorities of panellists supporting the introduction of a ‘sugar tax’ on sweetened drinks (59%) and regulation of fresh food pricing and supply, especially in rural and remote areas (55%).
There also appears to be strong community support for much broader preventative interventions that fundamentally alter where we live, with 72% of panellists supporting urban planning measures that encourage people to have a more active lifestyle by increasing the accessibility and safety of walking paths, cycling paths and public transport options in all communities. This indicates that there is community support for the Strategy to ‘aim high’ and pursue policies that will bring benefits to health through indirect pathways.
Conversely, the four least supported policy measures were all related to tobacco and alcohol, such as increasing and reforming taxes on these products, restricting the number of locations that sold alcohol or having public health campaigns to encourage people to quit smoking. This suggests that such measures will not have widespread support or popularity as initial ‘Focus Areas’ of the Strategy if broad community support and ‘buy-in’ for the Strategy is desired by government the initial priorities should be reconsidered. Indeed, it would appear that consumers have a strong desire to see action in new areas of health prevention as part of this Strategy rather than revisiting the areas that have been targeted for action over several decades.
Fig 4: graph - NatPrevHealth survey

When given the opportunity to suggest other specific policies or areas that should be included in the Strategy, consumers recommended a broad range of desired policies to be included in the 10-year plan. These included:
- Policies to address abuse, particularly domestic and child abuse, to prevent the devastating effects on both physical and mental health that can result from abuse.
- Policies that ensure the provision of school-based health education and health services, ensuring people are able to get the solid foundation they need to live a long and healthy life regardless of their personal circumstances.
- Policies that improve the training for health providers to promote and integrate preventative healthcare into normal health service provisions.
- Policies then ensure all Australians have a liveable wage, possible a Universal Basic Income, so that necessary healthcare can be afforded by all.
Policies that overhaul all oral and dental health so that it is no longer treated as an optional extra that people can ignore.
- Policies that support the development community spaces and groups that let people get the mental health support they need e.g. support hubs, shared gardens, ‘Men’s Sheds’ and young mothers groups.
When asked what items the National Preventative Health Strategy should use to measure its success against, five statistics were identified as being key by the majority of panellists (see Figure 5). Two of them were population-wide measures of specific health conditions, with a decrease in the number of people with chronic illness and a decrease in the number of people considered to be overweight/obese success measures supported by 73% and 64% of panellists respectively.
A further pair of measures of success supported by the panellists were about reducing the inequality between groups within the overall population, with panellists supporting a decrease in the rates of illness, disability and death in both disadvantaged communities (72%) and between different socioeconomic groups (72%). While the fifth measure that the majority (69%) of panellists supported was increasing the average number of ‘quality years’ lived in good health by people.
Fig 5: graph - NatPrevHealth survey
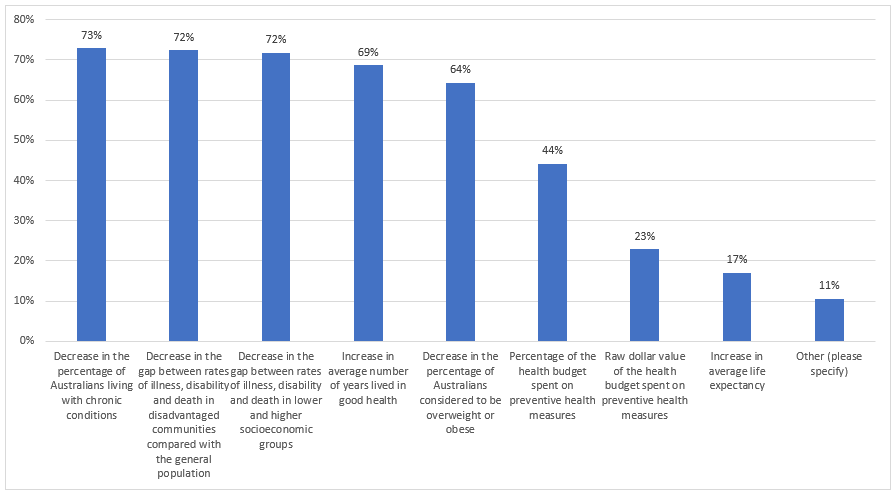
Collectively these measures highlight two areas that Australians prioritise and against which the success of the National Preventative Strategy will be measured: the ability for people to live a good life not just a long life and the ability for all Australian’s to be able to live healthily, not for some to be healthy and others to suffer.
Of note is that neither the raw dollar value of funds or the percentage of the health budget spent on preventative health were seen by the majority of panellists as an adequate measure of success, indicating that consumers want to see actual improvements in preventative health used to judge the Strategy’s success not the amount of action or work conducted by the government.
Success is avoiding hospitalisation and disease progression. Success should lead to savings in other parts of the healthcare system outside of the primary care/community/preventive areas. Start small and local; test effectiveness of intervention/promotion; then share and expand best practice to more locations. Success is having working collaborations and sharing of results.
- AHP Panellist
Conclusion and Next Steps
Preventative health is acknowledged by consumers as an area that is important and one in which Australia should, and can, do better. There was support from panellists for many of the proposals included in the draft Strategy, however there was also clearly a view that it does not go far enough. Consumers have an appetite for a more ambitious plan: less focus on items such as alcohol and tobacco, and a broader vision looking to address the crises in chronic illness and health inequities across Australia.
Ultimately this shows that while the draft Strategy is a step in the right direction, we still have a long way to go to fully embrace the full scope of preventative care in Australia.
CHF would like to thank all the panellists for contributing their time and views to this survey. We will use the results to shape our advocacy as a member of the National Preventative Health Strategy Expert Steering Group.
There are many conversations in this space, but sadly action to address NCDs and integrated care is still lacking. Time is of the essence! Health and well-being is a priority. We’ve seen how health/social can work together during the pandemic. Let’s continue this collaboration and get some real tangible action happening.
Funding needs to be committed for the long term and integrated into the ongoing health budget. There is no need to fund any more pilot projects or short-term strategies. There is sufficient evidence of what works but it needs real commitment and a good implementation approach including resourcing and in-built monitoring of outcomes in a 5 to 10-year program.
- AHP Panellist